What is a population-based approach to child welfare?
The child welfare system in the U.S. was built more than a century ago on the notion that children at risk of harm needed to be “rescued” from their parents in order to be safe. We now know that the opposite is true — in almost all cases, children need their parents in order to thrive. Sometimes, however, parents need help, especially when they are struggling with poverty, housing instability, mental health challenges, or substance use disorders. Experiencing maltreatment is traumatic enough for children. Separation from parents can compound that trauma, creating devastating effects that can span a lifetime.
A population-based approach to child welfare brings together stakeholders committed to a shared vision of promoting child and family well-being and ensuring that all families can access the supports they need to reach their potential. When an entire community shares the goal of family well-being, community members can work proactively to implement strategies that benefit everyone, rather than waiting and responding to individual needs. Such an approach prioritizes prevention before harm occurs and keeping families safely together. It leverages what we know about child development, brain science, interventions that demonstrate improved outcomes, and lessons learned from children and families with lived experience in the child welfare system.
The high cost of child maltreatment
Over the last few years, the overall child mortality rate in the U.S. has declined, but the number of child deaths due to abuse and neglect has increased.1 Every year, approximately 1,750 to 3,500 children die from child maltreatment.2 Of those deaths, 82% are children under age 5, and of those, more than half are babies who were in their first year of life.3 What’s more, child maltreatment fatalities have increased over the last several years.
The rate of child maltreatment is highest for children under age 1, and about half of all children entering foster care are 5 years old or younger. If removed and placed into care, children younger than age 1 also spend more time in care. This is particularly concerning because brain science shows these early years to be critical to a child’s healthy growth and development, and that nurturing, stable relationships during these formative years set the foundation for a child’s future.
The absence of these nurturing relationships and the presence of early adversity, also known as Adverse Childhood Experiences (ACEs), can have long-term impacts on multiple dimensions of health and well-being, such as mental health, chronic disease, infectious disease, risk behaviors, and life opportunities. ACEs include experiences such as: physical abuse, sexual abuse, neglect, growing up in a household with parental substance abuse, mental illness, or domestic violence. These experiences may result in contact with a child protection agency, but the impacts of ACEs hold true regardless of whether the agency becomes involved.
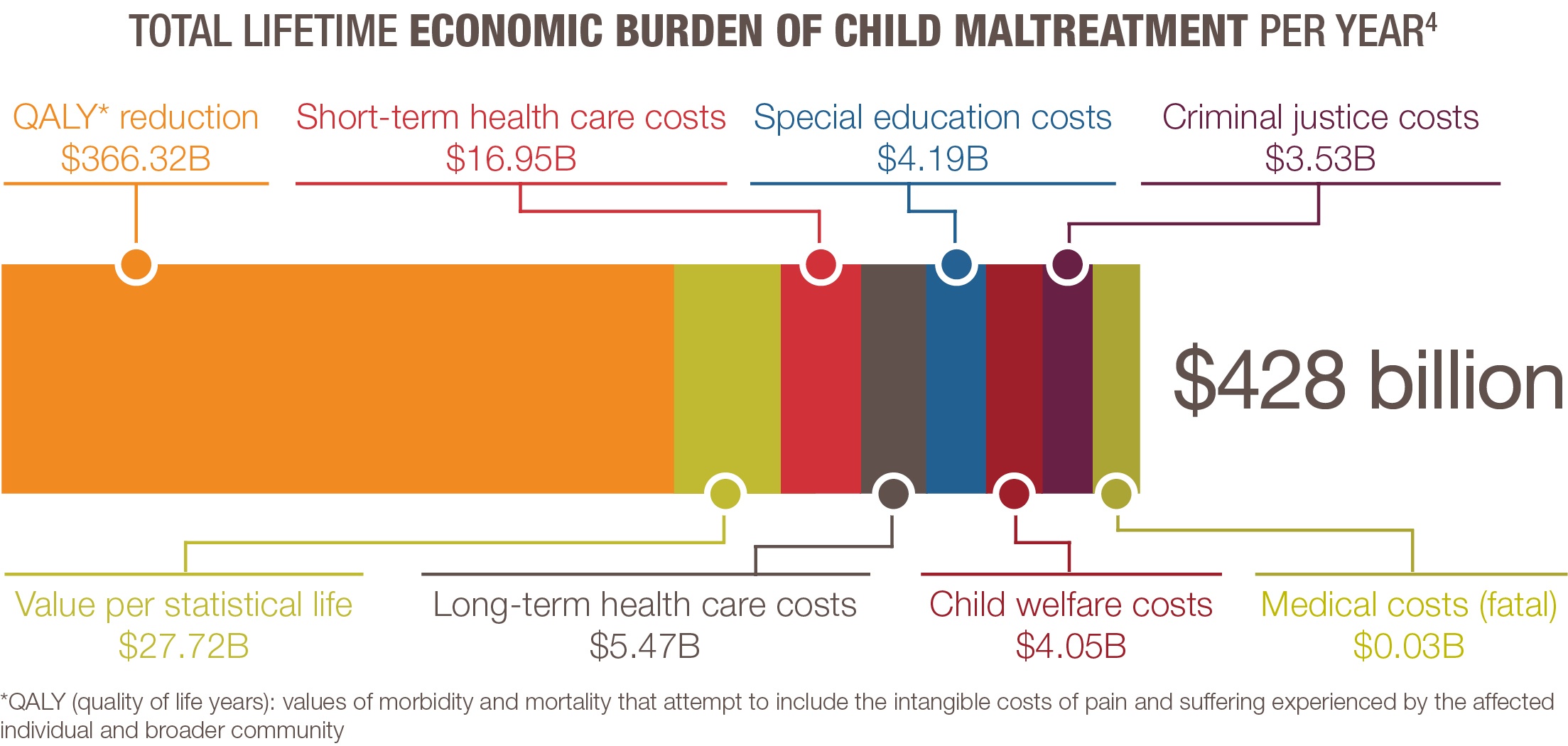
Child maltreatment and the conditions that can lead to it have direct impacts on health and well-being, both for the individuals involved and the community as a whole. In total, the lifetime economic burden resulting from new cases of child maltreatment in the U.S. is estimated to be approximately $428 billion each year. This estimate measures both the tangible costs associated with child abuse and neglect (such as costs related to medical care, special education, criminal justice involvement, etc.), in addition to the intangible costs of pain and suffering experienced by the child and the broader community. The cost burden is even greater for children who experience fatal child maltreatment, at $16.6 million per child.4
The role of the child protection agency
Protecting children is an important function in our society and there always will be a need for child protection agencies to fill this role. However, the scope of expected responsibilities for child protection agencies has expanded over time, exceeding their original mission and taxing their ability to effectively fulfill it. Child protection agencies often are expected to address myriad issues impacting the families they serve, including mental and behavioral health, substance use, domestic violence, homelessness, joblessness, and others. This is particularly challenging since the systems responsible for meeting those needs often do not work closely with the child protection agency or with each other. When each agency works in its own silo, children and families fall through the cracks.
The current child welfare system is rooted in investigation as a response to children that have already experienced abuse or neglect. In this construct, safety is defined as keeping children safe from further abuse and neglect once they already have experienced harm. While the child protection agency does have the critical responsibility of responding to allegations of child maltreatment and intervening when appropriate, it also has a role to play in the overall child welfare system to keep children safe and prevent harm in the first place. Ensuring child safety is further complicated by the public’s expectation that this is primarily the responsibility of the child protection agency, rather than seeing that every agency, every community, and every individual plays a critical role in keeping children safe.
The foster care system doesn’t need to exist the way it does right now. This is not a child safety crisis, it’s a poverty crisis, a racism crisis. … The majority of families I’ve worked with are really trying to figure it out. ‘How did I get here? How did this happen?’ We need to be a lot more focused on the larger society issues we’re trying to address.
– Jessica Chandler, Social worker and former youth in foster care featured in the movie, “Foster”
Building a population-based approach
A population-based approach to child abuse and neglect begins by identifying a community’s underlying needs, particularly those most widespread, and recognizes that child maltreatment is associated with a range of individual, family, and community-level factors. Stakeholders from various sectors of the community then work together to identify and implement strategies to effectively meet those needs at all levels. Initiatives that change the environments in which people live, creating healthier environments so that people’s default decisions and actions are better ones, will have a much more profound impact than a variety of programs targeting individual circumstances.
In contrast to the current child protection response, a population-based approach transforms the child welfare system by treating it as a continuum, with the child protection agency playing a clearly defined role alongside others. While a population-based approach to child welfare should include a partnership between the child protection agency and the public health agency, this is not enough. All sectors of a community must be engaged, including government agencies, community-based organizations, faith institutions, philanthropic organizations, and the business community, along with individual members of the community taking ownership for ensuring that all children are physically safe and emotionally nurtured.
In a transformed child welfare system, population-based strategies are prioritized in order to have the greatest impact, while still attending to the needs of those individuals who require higher levels of intervention. The Health Impact Pyramid below illustrates this shift.
In this pyramid, strategies to address socioeconomic risk factors, such as poverty and poor education, are at the base, and have the greatest potential population impact with the least individual effort. Examples of strategies to improve socioeconomic conditions for families include livable wage requirements, paid family leave, affordable housing, tax credits and affordable and accessible health insurance.5 Strategies addressing socioeconomic factors yield greater results because they target root causes or precipitating factors for subsequent downstream involvement with child protective services.6,7,8 The second tier aims to change the environmental context so that healthy decisions become the default rather than the exception, such as safe and walkable neighborhoods, access to subsidized high quality licensed child care, and universal preschool.
These first two tiers of the pyramid reflect the transformation that is needed in the current child welfare system — in order for all children to be safe and thriving, all families need to live in environments that are safe, stable, and nurturing. A 21st century approach reflects this change, moving the conversation from an individualized response to a preventive, population-based approach.
Moving up the pyramid to the third tier, long-lasting protective interventions seek to enhance an individual’s protective capacity but are generally less intensive than clinical interventions. At this point in the pyramid, interventions are still largely preventive but begin to shift toward reaching people as individuals rather than as a collective, and include strategies such as family resource centers, home visiting programs, and child injury prevention programs, for example safe sleep and water safety campaigns.
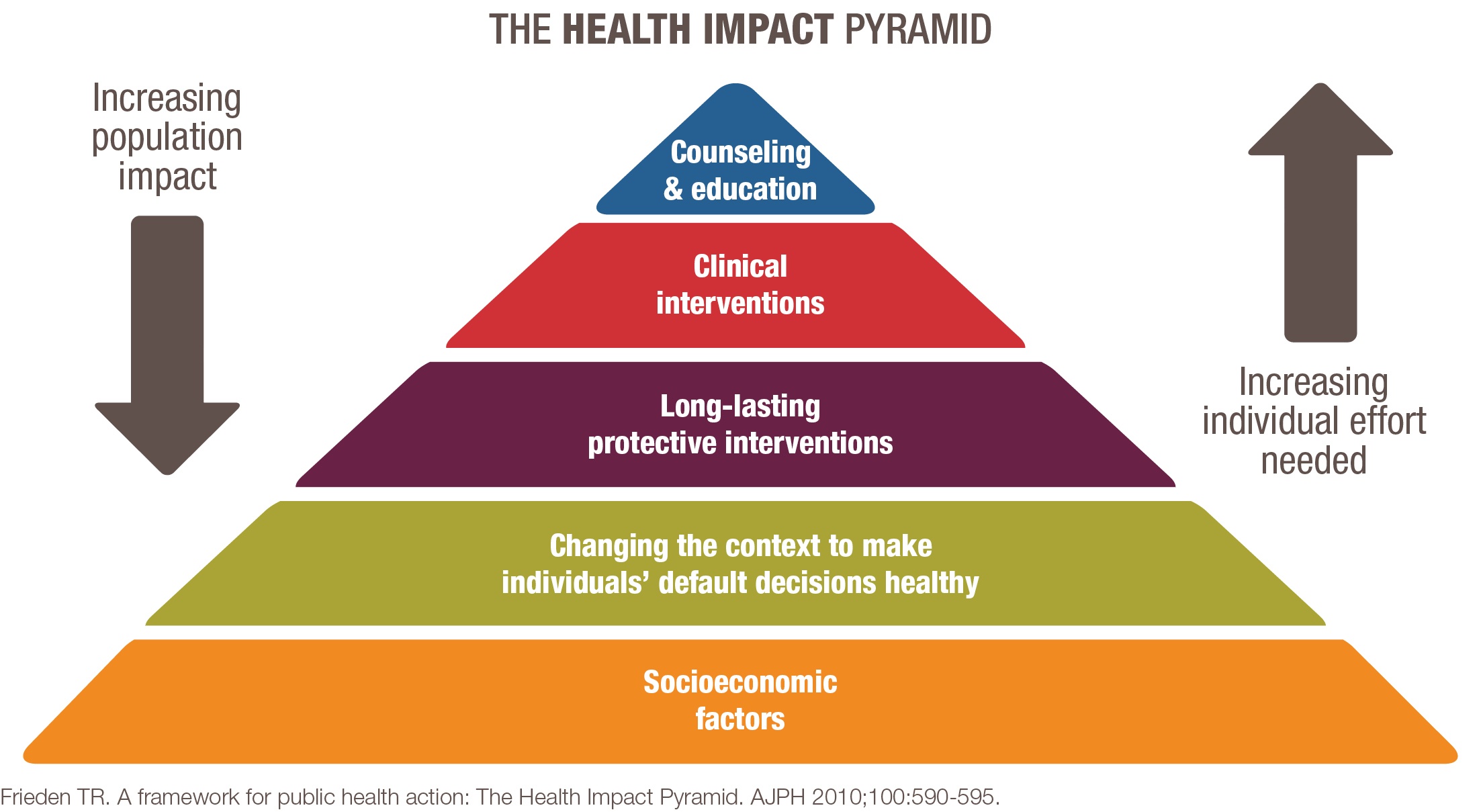
The final two tiers of the pyramid are much more focused on the individual and include intervening with children and families that already have experienced child abuse or neglect. For example, clinical interventions for children and families experiencing maltreatment may include neonatal abstinence support, differential response, improved risk and safety assessments, high quality legal representation, meaningful engagement with birth families, and high quality resource families (relative and non-relative). Counseling and education for children and families involved with the child protection agency may reflect evidence-based, trauma-focused clinical programs such as Trauma-Focused-Cognitive Behavioral Therapy, parent training programs such as Parent-Child Interaction Therapy and Parents as Teachers, and effective substance use treatment such as medication-assisted treatment and Motivational Interviewing. Although focused at the individual level, these interventions could have a large impact on the overall population if they are applied across the board with fidelity.
The strategies within the Health Impact Pyramid cannot be implemented by the child protection agency alone. A transformed child welfare system requires the collective efforts of all sectors and individuals in society, and that each partner recognizes the urgency of this work. Our current approach to child welfare is not serving families well, and children are being harmed and even dying as a result. A transformed child welfare system shifts the focus of child safety from intervention to prevention, and seeks to support and serve all families so that every child can thrive.
People want to help children without really understanding that children live in a family, and a family resides in a community, and a community is within a broader society that either has policies and a context that supports their health and well-being, or one that makes achievement of health and well-being difficult for some or many to achieve.
– Dr. Melissa T. Merrick, former senior epidemiologist, National Center for Injury Prevention and Control, Centers for Disease Control and Prevention
Resources
1 Annie E. Casey Foundation. (2019). Kids count data center: Infant mortality in the United States. Retrieved from https://datacenter.kidscount.org/data/tables/6051-infant-mortality#detailed/1/any/false/871,870,573,869,36,868,867,133,38,35/any/12718,12719
Annie E. Casey Foundation. (2019). Kids count data center: Child and teen death rate in the United States. Retrieved from https://datacenter.kidscount.org/data/tables/7243-child-and-teen-death-rate?loc=1&loct=1#detailed/1/any/false/871,870,573,869,36,868,867,133,38,35/any/14285,17513
2 Commission to Eliminate Child Abuse and Neglect Fatalities. (2016). Within our reach: A national strategy to eliminate child abuse and neglect fatalities. Retrieved from https://www.acf.hhs.gov/sites/default/files/documents/cb/cecanf_final_report.pdf
3 Children’s Bureau. (2017). Child maltreatment 2017. Retrieved from https://web.archive.org/web/20201125124338/https://www.acf.hhs.gov/sites/default/files/cb/cm2017.pdf
4 Peterson, C., Florence, C. & Klevens, J. (2018). The economic burden of child maltreatment in the United States, 2015. Child Abuse & Neglect, 86, 178-183.
5 Strategies in this section were shared by Teresa Covington, Director of Within Our Reach, Alliance for Strong Families and Communities. They are not exhaustive and are offered only as examples for consideration.
6 Sedlak, A.J., Mettenburg, J., Basena, M., Petta, I., McPherson, K., Greene, A., and Li, S. (2010). Fourth National Incidence Study of Child Abuse and Neglect (NIS–4): Report to Congress, Executive Summary. Washington, DC: U.S. Department of Health and Human Services, Administration for Children and Families.
7 Font, S., and Warren, E. Inadequate housing and the child protection system response. Children and Youth Services Review, 35 (2013), 1809-1815.
8 Maguire-Jack, K. and Font, S. Intersections of individual and neighborhood disadvantage: Implications for child maltreatment. Children and Youth Services Review, 72 (2017), 44-51.